The FDA’s Project Optimus initiative has fundamentally reshaped oncology dose optimization by shifting development away from traditional maximum tolerated dose (MTD)-based paradigms toward mechanism-driven dose selection strategies. Translational pharmacokinetic-pharmacodynamic (PK/PD) modeling provides a critical quantitative framework for linking tumor drug exposure with pharmacodynamic activity, biomarker response, and clinical outcomes. Modern approaches integrate physiologically based pharmacokinetic (PBPK) modeling, biomarker-guided pharmacology, and advanced computational frameworks to support rational dose optimization and improve clinical translation.
This whitepaper examines key challenges in translational PK/PD implementation, including tumor heterogeneity, biomarker integration, and clinical variability. It further outlines emerging mechanistic modeling strategies—including PBPK, PK/PD, and Quantitative Systems Pharmacology (QSP) approaches—and provides strategic considerations for building integrated translational capabilities aligned with the evolving Project Optimus era of oncology drug development.
The development of cancer therapies is becoming increasingly complex due to tumor heterogeneity and the rise of novel treatment modalities. Traditional dose selection frameworks—originally designed for cytotoxic chemotherapies—often result in molecularly targeted therapies entering registration trials with insufficiently characterized dosing and scheduling. The long-standing maximum tolerated dose (MTD) approach does not adequately reflect the intricate dose–response relationships seen with targeted agents, immunotherapies, and combination treatments. As limitations of this approach become more evident, the need for more informed, biology-driven dose selection strategies is gaining prominence.
Project Optimus promotes improved strategies for dose finding and optimization by integrating both nonclinical and clinical evidence into dose selection, including the use of randomized dose-ranging studies. The field is moving away from reliance on MTD toward precise identification of the Optimal Biologic Dose (OBD). This shift in regulatory thinking highlights a deeper scientific recognition that optimizing the therapeutic index depends on understanding drug mechanisms rather than relying solely on empirical dose escalation.
Recent evidence indicates a clear evolution in early-phase trial designs, with greater use of Bayesian methods and structured dose-optimization frameworks. Modern oncology drug development requires the integration of diverse datasets to rigorously define dose–exposure–response relationships with adequate mechanistic insight for regulatory evaluation. Given the typically narrow therapeutic windows of anticancer agents, more refined PK/PD modeling is essential for accurately determining first-in-human dosing.
Physiologically Based Tumor Disposition
Tumor exposure prediction represents one of the most technically challenging aspects of translational PK/PD modeling. Factors such as tumor blood flow, vascular permeability, interstitial transport, extracellular matrix composition, and dynamic changes in the tumor microenvironment significantly influence drug distribution within tumor tissue. Unlike systemically distributed drugs, oncology compounds encounter unique challenges including heterogeneous vascularization, variable tissue penetration, and evolving tumor physiology during treatment.
Physiologically Based Pharmacokinetic (PBPK) modeling serves as a valuable tool for forecasting drug behavior by mechanistically characterizing drug disposition and estimating pharmacokinetic parameters. Successful PBPK model development requires species-specific anatomical and physiological data along with compound-specific pharmacokinetic properties and tissue partition coefficients.
Modern PBPK approaches incorporate tumor-specific physiological parameters including blood flow (typically 0.1–0.3 mL/min/g), vascular permeability, and interstitial transport kinetics. Key validation strategies include imaging-based confirmation of tumor blood flow, ex vivo assessment of tissue binding, and receptor expression quantification. PBPK modeling can be effectively applied across multiple stages of oncology drug development.
Pharmacodynamic (PD) biomarkers play a central role in linking drug exposure to pharmacological response during translational drug development. These biomarkers quantitatively measure biological processes linking drug administration to pharmacological effect, including target engagement, downstream physiological changes, and clinical response. Successful translational programs integrate target engagement biomarkers with pathway response indicators to create multidimensional understanding of drug mechanism and efficacy.
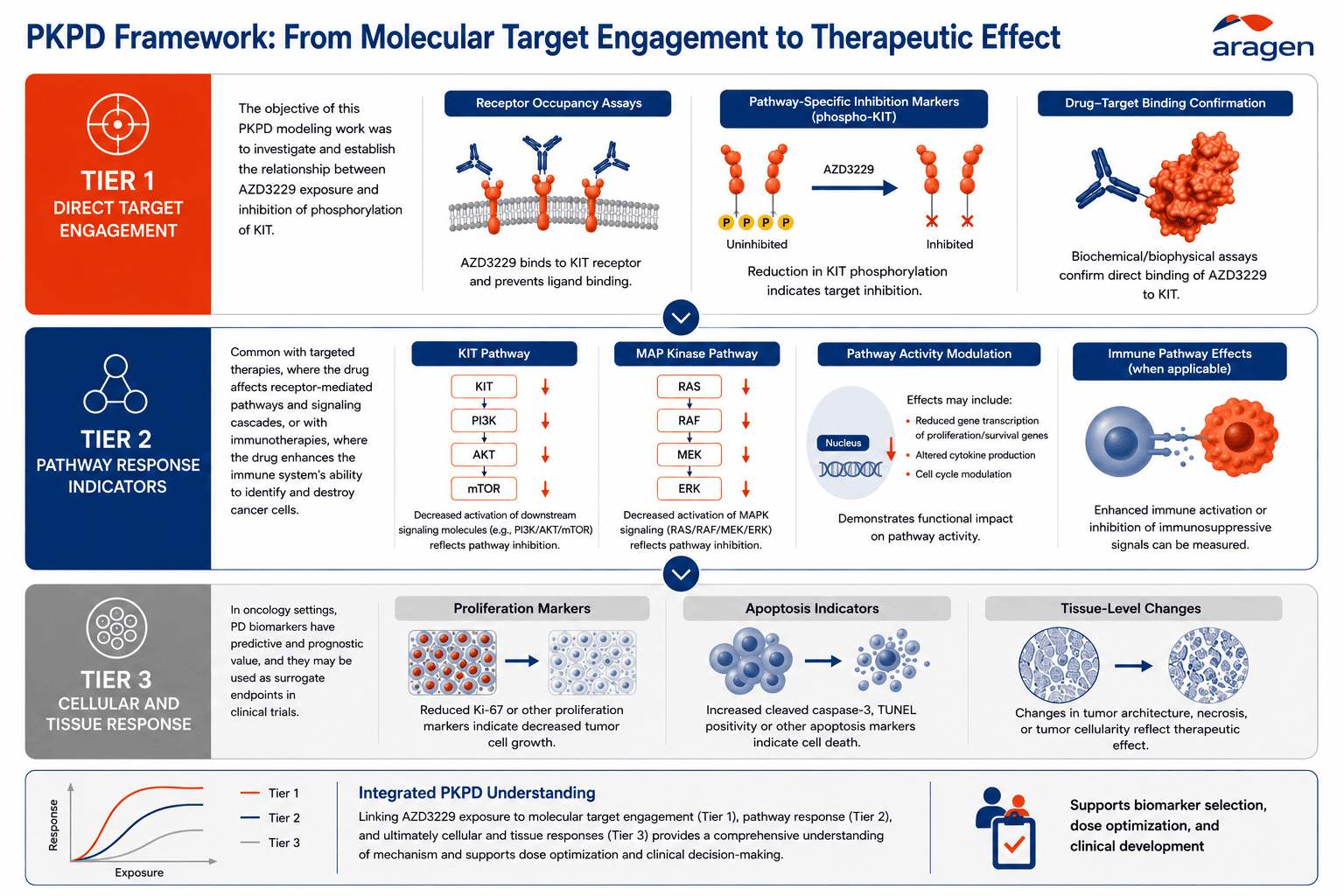
Figure 1: Three-Tier Biomarker Strategy Framework. It shows hierarchical biomarker selection from direct target engagement through pathway response to clinical outcomes, with examples and validation requirements for each tier.
Temporal changes in tumor biology and treatment response present significant challenges in translational PK/PD modeling. Xenograft models have contributed substantially to model development; however, their ability to fully recapitulate the human tumor microenvironment and predict clinical outcomes remains limited. Clinical translation is further complicated by sparse patient data, limited PK sampling, and pronounced tumor heterogeneity.
To address these complexities, population pharmacokinetic approaches are increasingly applied to characterize inter-patient variability in oncology populations. Integrated PK-covariate models can predict individual drug exposure using biomarker data and improve forecasts through sparse sampling strategies, thereby supporting precision dosing and personalized treatment optimization.
Quantitative Systems Pharmacology (QSP)
Mechanistic modeling approaches are increasingly used to bridge molecular drug action with clinical outcomes in oncology. Quantitative Systems Pharmacology (QSP) represents the most comprehensive framework for complex oncology drug action, integrating cellular target engagement with tissue-level tumor dynamics and patient-level clinical responses. PBPK–PD and QSP approaches are mechanistic, bottom-up frameworks that encompass simpler PK–PD models as subsystems. While simplified models may be adequate for applications such as dose optimization, more complex QSP models are particularly valuable when underlying disease or drug mechanisms remain incompletely understood.
Hybrid Translational Approaches
Hybrid modeling strategies combine mechanistic understanding with clinical observations to improve translational predictability. In these approaches, hybrid PK/PD models integrate mechanistic tumor biology with clinical pharmacokinetic data while enabling continuous model refinement using emerging clinical observations. This integrated framework has been successfully applied in preclinical and clinical tumor growth inhibition models, where average drug concentration per treatment cycle has been shown to predict tumor response, supporting schedule-independent efficacy assessment and treatment optimization.
Clinical Translation and Predictive Modeling
Integrated modeling approaches are increasingly used to support clinical decision-making for complex oncology therapeutics. By combining systemic pharmacokinetics with patient-specific tumor growth parameters, integrated PK-PD models can be translated from preclinical settings to the clinic. Clinical trial simulations have shown that progression-free survival rates predicted from translated models closely align with observed outcomes, demonstrating the practical value of mechanistic modeling frameworks for optimizing therapeutic strategies.
Retrospective analyses have demonstrated the utility of translational PK/PD modeling in predicting clinically active human doses, with mechanistic modeling approaches contributing to improved development efficiency. In oncology, the high prevalence of non-responders and the rising cost of therapy further emphasize the need for model-informed strategies, including PK-guided dose optimization and precision dosing approaches.
The growing regulatory acceptance of mechanistic modeling is reflected by the approval and breakthrough therapy designation of multiple anticancer agents supported by PBPK analyses. Regulatory agencies, including the FDA, also encourage early scientific engagement through pre-IND and Type C meetings for programs incorporating robust mechanistic models.
Effective translational PK/PD implementation requires coordinated integration of discovery biology, bioanalytical sciences, clinical pharmacology, and biostatistics expertise. These modeling approaches provide critical insight into pharmacological modulation dynamics and support informed decision-making for dose selection and optimization strategies.
PBPK modeling is now widely accepted by the FDA for regulatory decision-making and employs a mechanistic “bottom-up” framework that complements traditional empirical “top-down” PK approaches. Supporting these capabilities increasingly requires advanced computational infrastructure capable of handling complex model development, simulation workflows, and integration of diverse preclinical and clinical datasets.
Aragen enables mechanistic dose optimization through an integrated translational approach. It begins with physiologically based tumor disposition, where Aragen develops PBPK models incorporating tumor-specific parameters including blood flow, vascular permeability, and interstitial transport kinetics and validates them using in vitro, in vivo, imaging data, and IVIVE-based extrapolation to support accurate first-in-human dose prediction.
Building on this, biomarker integration and target engagement are supported through advanced bioanalytical capabilities and tiered biomarker strategies, spanning direct target engagement, pathway response, and clinical outcome indicators to quantitatively link drug exposure with pharmacodynamic response across small molecules, biologics, and novel modalities.
To address temporal variability, resistance mechanisms, and tumor heterogeneity, Aragen applies population PK and covariate modeling incorporating sparse sampling strategies, enabling robust exposure–response characterization and supporting precision dosing and personalized treatment optimization.
These insights are further strengthened through integrated PK/PD and QSP frameworks, where hybrid models combine mechanistic tumor biology with clinical pharmacokinetic data, enabling schedule-independent efficacy assessment via tumor growth inhibition modeling, predictive clinical trial simulations forecasting progression-free survival, and continuous model refinement using emerging clinical observations.
Finally, Aragen translates these insights into clinical decision support, facilitating model-informed dose selection, Optimal Biologic Dose identification, and trial optimization—while supporting regulatory-aligned strategies under Project Optimus through pre-IND and Type C meeting packages leveraging mechanistic modeling evidence acceptable to FDA.
The shift toward mechanistic dose optimization is reshaping modern oncology drug development. Integrated PK–PD, PBPK, and QSP modeling frameworks provide quantitative understanding of the relationships between drug exposure, tumor biology, biomarker dynamics, and clinical response, enabling more informed therapeutic decision-making. Organizations adopting advanced translational modeling capabilities are increasingly positioned to drive precision oncology development.
Project Optimus has accelerated the transition away from traditional maximum tolerated dose (MTD)-based development strategies by emphasizing clinically optimized dosing approaches. As oncology therapeutics become increasingly complex, future success will depend on the ability to integrate mechanistic modeling, translational data, and clinical insights to improve dose selection, predict therapeutic outcomes, and support precision medicine strategies.
Aragen Life Sciences provides integrated translational PK/PD capabilities specifically designed for oncology drug development programs. Our experienced in vivo pharmacology team maintains strong domain expertise across validated oncology, inflammation, autoimmune disease, and fibrosis models, supporting mechanistic biomarker development and target engagement assessment essential for translational modeling success.
Our comprehensive DMPK infrastructure evaluates drug-like properties across all development stages, while biomarker identification and validation platforms including qPCR, flow cytometry, high-content imaging, and LC-MS/MS support sophisticated pharmacodynamic endpoint development. The InCoRe platform coordinates real-time data sharing and analysis across functions, enabling the cross-functional collaboration essential for effective translational modeling.
With 19,000+ GLP studies completed and global regulatory submission expertise, Aragen delivers IND-ready translational packages that support FDA Project Optimus requirements while maintaining the mechanistic rigor demanded by modern oncology development programs.
Ready to discuss your translational PK/PD programme? Contact us today to accelerate dose optimization and clinical translation through integrated modeling strategies.